GP Surgeries in Cookstown and Magherafelt is one of 9 surgeries to benefit from funding from the Northern Heath & Social Care Trust.
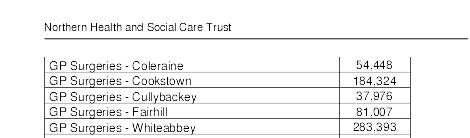
The Trust have allocated £1,138,154 for improvements to surgeries across the Trust Cookstown Surgery will receive £184,234 in funding while Fairhill in Magherafelt will receive a very much needed £81,007.
The Trust have allocated £1,138,154 for improvements to surgeries across the Trust Cookstown Surgery will receive £184,234 in funding while Fairhill in Magherafelt will receive a very much needed £81,007.
For full accounts contact Save The Mid


 RSS Feed
RSS Feed
