A&E performance March 2013 - ref DHSSPS
Between March 2012 and March 2013:
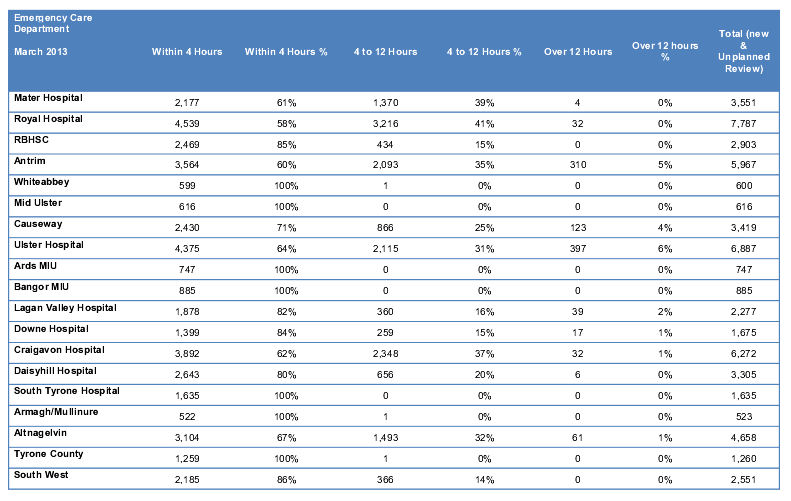
- In Type 1 emergency care departments, the percentage of patients attending that were either treated and discharged home or admitted within 4 hours decreased by 5.3 percentage points, from 71.6% to 66.3% ).
- In Type 2 emergency care departments, the percentage of patients attending that were either treated and discharged home or admitted within 4 hours decreased by 4.6 percentage points, from 87.5% to 82.9% .
- In Type 3 emergency care departments, the percentage of patients attending that were either treated and discharged home or admitted within 4 hours remained at 100.0%.
- The number of patients that waited longer than 12 hours to be either treated and discharged home, or admitted, increased slightly (34, 3.4%) from 987 to 1,021. In particular, performance declined notably at the Ulster between January and March, from 223 to 397.

 RSS Feed
RSS Feed
