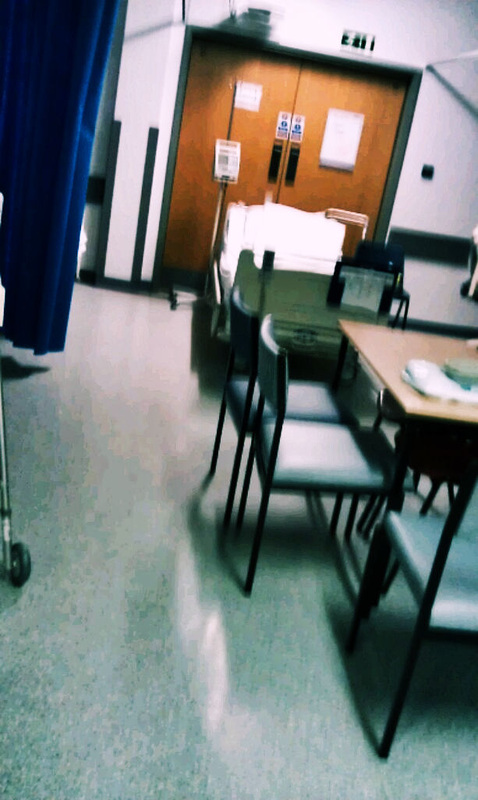
Bed placed in ward C3 that is blocking fire door. Amended 19/03/2013
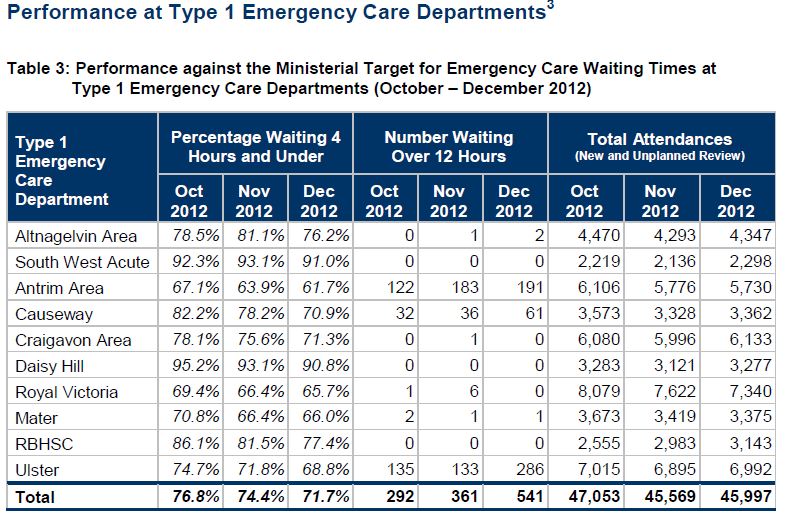
496 patients wait over 12 hours in A&E during Oct-Dec 2012
For 5 years running the performance of Antrim A&E has been far below standards, not only did it fail to treat 95% of patients in under 4 hours, it failed to meet that target in 8 hours. It does not matter if the number of people waiting 12 hours or more has decreased, no-one should have to wait that long in any instance of acute care in this day and age.
This is directly related to the capacity of Antrim Hospital, which only ever seen the building on one of its 2 phases, beds are now placed in any free space in the hospital and also in front of fire exits.
We have seen a corridor turned into a ward, extra beds that were called show beds put into wards to create extra capacity and now we see what the Trust call escalation beds placed in front of fire exits, what exactly is it going to take for anyone in a position of power to finally reprimand the trust for the actions"
The new A&E and 24 bed single room ward will not solve this problem, it does not matter how big an A&E they build in Antrim if inpatients is not increased accordingly.
At the most recent board room meeting within the Trust the crisis was discussed:
Last year Valerie Jackson said 90% of people were waiting because there was no beds to admit them, the new director for acute said the same, beds are the problem. Chairman and Sean Donaghy said the fire service ok'ed the blocking of the fire doors, then changed their mind to say internal health and safety.
Either way no matter how big the new A&E is at Antrim we will still see serious issues as the hospital inpatient capacity is not big enough to meet demand.
The operational capacity of the Trust can very quickly be remedied by reopening the Mid Ulster hospital for intermediate care, this option should fully be explored and support by all representatives in the Trust area. Shutting down 97 beds in Mid Ulster has increased problems at Antrim as it was not extended to cope with these closures.
For 5 years running the performance of Antrim A&E has been far below standards, not only did it fail to treat 95% of patients in under 4 hours, it failed to meet that target in 8 hours. It does not matter if the number of people waiting 12 hours or more has decreased, no-one should have to wait that long in any instance of acute care in this day and age.
This is directly related to the capacity of Antrim Hospital, which only ever seen the building on one of its 2 phases, beds are now placed in any free space in the hospital and also in front of fire exits.
We have seen a corridor turned into a ward, extra beds that were called show beds put into wards to create extra capacity and now we see what the Trust call escalation beds placed in front of fire exits, what exactly is it going to take for anyone in a position of power to finally reprimand the trust for the actions"
The new A&E and 24 bed single room ward will not solve this problem, it does not matter how big an A&E they build in Antrim if inpatients is not increased accordingly.
At the most recent board room meeting within the Trust the crisis was discussed:
- A&E escalated between 1st Jan - 9th Jan with the worst period being 5th & 6th & 7th.
- The flash point before that was Christmas eve and the hospital had not recovered.
Last year Valerie Jackson said 90% of people were waiting because there was no beds to admit them, the new director for acute said the same, beds are the problem. Chairman and Sean Donaghy said the fire service ok'ed the blocking of the fire doors, then changed their mind to say internal health and safety.
Either way no matter how big the new A&E is at Antrim we will still see serious issues as the hospital inpatient capacity is not big enough to meet demand.
The operational capacity of the Trust can very quickly be remedied by reopening the Mid Ulster hospital for intermediate care, this option should fully be explored and support by all representatives in the Trust area. Shutting down 97 beds in Mid Ulster has increased problems at Antrim as it was not extended to cope with these closures.
Question that was raised with the NHSCT on 24th Jan 2013 from save the mid
I would like to have created more informed questions however due to the dumbing down of the performance report to make serious issues look better I will try my best to come straight to the point: A&E performance, it is suggested that the A&E was in surge capacity in the previous board meeting, this is untrue, according to the performance report Antrim A&E only seen 62% of patients in under 4 hours with Causeway only meeting 71% (page 10) . Cumulative A&E activity across the NHSCT for A&E activity (page 43) has increased by 192 patients, with Antrim seeing a decrease of 257 patients, Causeway a decrease of 256 patients and Whiteabbey a decrease of 96 patients. Mid Ulster has seen an increase of 801 patients the only facility that is breaking the trend. The cumulative attendance at type 1 A&E’s within the trust is – 513. What is missing from the performance report is the amount of patients admitted via A&E, for the month of Nov 11 the Trust collectively seen the highest amount of patients admitted via A&E in a 2 year analysis, it can be clear that these patients were not admitted for no reason as the A&E in Antrim is having consult led admission vetting, also the GP out of hours is operational.What is the problem with A&E? Why still is performance at an all-time low, why are show beds blocking fire exits, what are the clinical risk involved in having show beds for acute patients and what is the health and safety risk of blocking fire exits?
- · It can be identified that there is no surge capacity, from previous performance reports, the old style layout would have shown this.
- · It can be identified that admissions via A&E are closing scrutinised by consultants and only those requiring admission are being admitted.
- · It can be identified form the operational side of Antrim hospital that show beds are covering fire exits and the wards are overcrowded & that day case beds have been used for inpatients, I was in the hospital I seen this with my own eyes and have photographic proof.
- · It can be identified the attendance for the month of December was the lowest in the 3 month period as stated within the report. I see that admissions via has been removed from the report, a useful tool when trying to determine performance.
Does the board seriously believe that a new A&E, or pathways will solve the problem of a full hospital?
Summary of key performance indicators;
Governance
Patients Safety. Throughout 2012/13 NHSCT will continue to progress towards the full implementation of approved quality improvement plans and the achievement of Trust-specific targets for ventilator associated pneumonia, surgical site infection, central line infection, the crash calls rate
and mental health inpatient care. A summary of progress is presented in section 3.0, including summarised narratives.
The HCAI Performance Report demonstrates the Trust's performance against regional targets and our performance in other areas related to the reduction of health associated infections; these are hand hygiene compliance, environmental cleanliness scores, anti-microbial prescribing and High
Impact Interventions.
This information is presented in Section 3.1
Complaints received for November 2012 totalled 75, with 47 (63%) being responded to within 20 working days. The target for 2011/12 was 72% within 20 working days and the Trust achieved 72%. The position for November is not yet available.
Patients waiting in A&E over 12hrs for treatment must be reported as Serious Adverse Incidents under DHSSPS guidance. There were 252 cases reported to DHSSPS for December 2012. 14 of these cases were related to ambulance breaches which were attributed to the Trust. This excludes breaches which were already attributed to the Ambulance Service.
HR/Staffing: The cumulative 2012/13 absence position at the end of November was 5.50%, which is above the interim target of 5.0% for 12/13. The cumulative position for 11/12 was 5.32%.
Access Targets/Waiting Times
With significant financial pressure and requirement for savings it has been necessary to continue with financial restrictions within the Trust. This has impacted on waiting times targets. The HSCB has provided additional funding for quarter 1 and 2 to achieve backstops by September 12; and is currently in the process of agreeing additional funding for Quarter 3 and 4. This will assist in
improving backstop positions and commissioner targets. This extra funding will be allocated to additional In-house and Independent Sector activity.
Elective In-patients and daycases – As at the 31st December there were 1,038 NHSCT patients waiting over 13 weeks, 534 of which are IS transfers.
As at the 31st December 88% of patients were waiting within the Trust Plan backstop positions. 690 patients were breaching the backstop positions, 50 of which were core endoscopy patients and 50 were IS transfers. 82% of total patients were waiting within 13 weeks. (Information validated weekly
by operational staff). New backstops have been applied for quarter 3, 2012/13.
Out-patients - As at the 31st December there were 2,954 NHSCT patients waiting over 9 weeks, 1,084 of which are Independent Sector (IS) transfers.
As at the 31st December 80% of outpatients were waiting within the Trust Plan backstop positions with 2,615 patients breaching the backstop. An additional 24 patients were waiting over 9 weeks for ICATS specialties. (Information validated weekly by operational staff) New backstops applied for quarter 3 2012/13.
Diagnostics – As at 31st December there were 1,484 Cardiology patients, 3 Respiratory Physiology patients and 16 Urodynamic patients waiting over 9 weeks. An action plan is in place to deliver the 9 week target by January ’13.
AHPs - As at 31st December there were 234 patients waiting over 9 weeks, 201 Occupational Therapy, 11 Physio and 22 Speech & Language. SLT are expecting to have no breaches by the end of March ‘13. Other AHPs are expecting to have no breaches by the end of February ’13.
Mental Health waiting list – As at 31st December, there were 57 (CAMHS) patients in breach of the 9 week target. Psychological Therapies continues to be monitored against the 13 week target and there were 24 patients in breach of this target.
Cancer Services: 98% Patients diagnosed with Cancer should commence treatment within 31 days of decision to treat. In addition to this target, 95% of patients urgently referred with suspected cancer should begin first
definitive treatment within 62 days. Latest information up to 14th December shows that 100% has been achieved for the 31 day target and 85% has been achieved for the 62 day target, for November. (This position can change as patient records become updated).
Suspected Breast Cancer patients referred urgently should be seen within 14 days of referral. Monthly reports are provided in Table 11 (Access / Waiting Time Targets Section) with December 2012 having 100% seen within 14 days.
Accident & Emergency: All patients should be seen within 12 hours. During December the Trust had 252 patients in excess of this target. 14 of these breaches were requests to the NI Ambulance Service (NIAS) outside of a 4
hour request target. Within the overall Trust A&E sites there were 68% of patients who had been seen and discharged within 4 hours for December. The target is 95% at each individual site. Both Antrim (62%) and Causeway (71%) sites continue to fall below the target. An Unscheduled Care Programme Board has been setup including an Improvement group to identify and implement actions for A&E.
Responsibility for 12-hour breaches for patients who require ambulance transport from the Emergency Department is as follows: - Where a patient requiring NIAS transport from the Emergency Department waits longer than 12
hours, the breach will be attributed to NIAS if the transport was requested within four hours of the patient presenting to the Emergency Department. - If however the request for ambulance transport is made after four hours of the patient presenting at the Emergency Department, the breach will be attributed to the relevant Trust.
Community Care Services: 90% of complex cases are to be discharged from hospital with a suitable care package within 48 hours of being determined medically fit. The Trust has achieved 84% for December. For noncomplex
cases the target remains 100% within 6 hours. The Trust has achieved 96%. All other discharges should be achieved within seven days. The Trust had 11 patients which waited over seven days during December (Antrim 8 patients - longest wait was 39 days, Causeway 1 patient – longest wait was 36 days and Mid Ulster 2 patient – longest wait was 9 days).
Older people with continuing care needs should wait no longer than eight weeks for assessment to be completed and have the main components of their care needs met within a further 12 weeks. At the 31st December the Trust achieved 100% of clients being assessed within 8 weeks and 99% having had their main care components met within 12 weeks.
 RSS Feed
RSS Feed
