Another winter break and yet again another winter breakage of our emergency care system, one would be forgiven for thinking that this occurs only at Christmas however this seems to be the only time the media converges on the A&E issue, however what happened was entirely predictable and to a point preventable.
It was not predictable because it happens every year, it is predictable because it happens every month, there has not been much improvement in our emergency care system since December last year. ( https://www.health-ni.gov.uk/sites/default/files/publications/dhssps/hs-nitws-ecwt-tables_0.csv )
It was not predictable because it happens every year, it is predictable because it happens every month, there has not been much improvement in our emergency care system since December last year. ( https://www.health-ni.gov.uk/sites/default/files/publications/dhssps/hs-nitws-ecwt-tables_0.csv )

Including last Christmas right up to September 2017 over 7,000 people waited over 12 hours in A&E’s, the media did largely ignore this by buying into the Bengoa reform and Michelle O’Neill’s 10-year plan. 10 years gives good cover to dodge any current issues though this plan did not include anything we have not seen before, it only furthered a conversation.
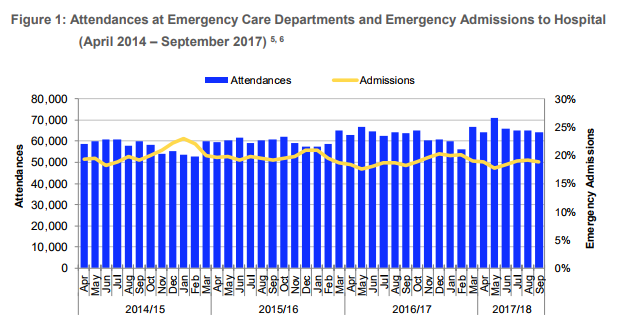
The Department of Health, Health & Social Care Board and all Health Trusts knew that the winter of 2017/18 was going to see a rise in attendances after seeing a rise in attendances all year, the main question that needs to be answered is where was the preparation? Every year the same excuse will come out, the A&E’s see an unprecedented amount of people, this year it was a 3.7% increase from last year. While the PR from the HSCB will say it’s a 15% rise over 2 years this should not matter as the rise 2 years ago should already have been factored into any planning for this year.
Now let’s recap on what has made the news this year during the crisis versus what is happening all year around, below are example of what happens during the Winter crisis compared to other examples that happen all year around:
The Department of Health, Health & Social Care Board and all Health Trusts knew that the winter of 2017/18 was going to see a rise in attendances after seeing a rise in attendances all year, the main question that needs to be answered is where was the preparation? Every year the same excuse will come out, the A&E’s see an unprecedented amount of people, this year it was a 3.7% increase from last year. While the PR from the HSCB will say it’s a 15% rise over 2 years this should not matter as the rise 2 years ago should already have been factored into any planning for this year.
Now let’s recap on what has made the news this year during the crisis versus what is happening all year around, below are example of what happens during the Winter crisis compared to other examples that happen all year around:
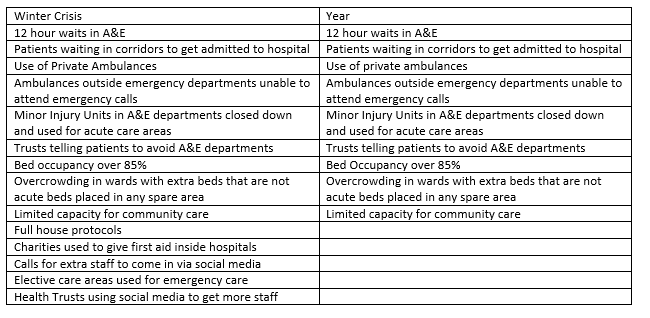
Does this look like we had plans made? Beds and staff should have been a number 1 priority but having to call in charities to give first aid shows that there were no staffing plans in at least 2 Trusts. Social media calls for nurses? In a way this was an attempt by the Trust to shame nurses into going into work, in the past I have seen the messages sent to nurses by managers, these messages usually come in the form of a text message, why the Trust used social media this time to contact staff instead of directly contacting them in very questionable.
As per usual when addressing these issues, the Dept. Of Health will come out and mainly say that people are using A&E inappropriately, so I put it to the Department provided the figures of people who should not have attended, not a made up % of maybes but an actual tangible figure.
There is a huge difference between people who attend who could have got treated elsewhere and saying that they should not be there, the Royal College of Emergency Medicine do say roughly 15% of attendees to A&E could be treated elsewhere, but this is only after the patient has been triaged and this 15% in all essence can be treated quickly and sent home in any functional system. For example, there is a dedicated Minor Stream in Antrim so that patients with less serious illnesses can be treated and sent home, the only problem is that this newish state of the art A&E cannot deal with the amount in its major’s stream so it must take over the minor stream.
Below shows the difference between people who attend versus people who are sent home, this would broadly be in line with the Royal Colleges percentage and does not show a mass of people attending who don’t need to be there. What the table does show is that even with an increased threshold for admissions it is the summer months that sees more people attend A&E that do not need admission. (https://www.health-ni.gov.uk/sites/default/files/publications/health/hs-niwts-ecwt-q2-17-18.pdf)
As per usual when addressing these issues, the Dept. Of Health will come out and mainly say that people are using A&E inappropriately, so I put it to the Department provided the figures of people who should not have attended, not a made up % of maybes but an actual tangible figure.
There is a huge difference between people who attend who could have got treated elsewhere and saying that they should not be there, the Royal College of Emergency Medicine do say roughly 15% of attendees to A&E could be treated elsewhere, but this is only after the patient has been triaged and this 15% in all essence can be treated quickly and sent home in any functional system. For example, there is a dedicated Minor Stream in Antrim so that patients with less serious illnesses can be treated and sent home, the only problem is that this newish state of the art A&E cannot deal with the amount in its major’s stream so it must take over the minor stream.
Below shows the difference between people who attend versus people who are sent home, this would broadly be in line with the Royal Colleges percentage and does not show a mass of people attending who don’t need to be there. What the table does show is that even with an increased threshold for admissions it is the summer months that sees more people attend A&E that do not need admission. (https://www.health-ni.gov.uk/sites/default/files/publications/health/hs-niwts-ecwt-q2-17-18.pdf)
Below we see the difference in time spent in A&E for people who need admission and for people who are sent home in the latest stats June to sept 2017.
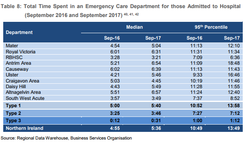
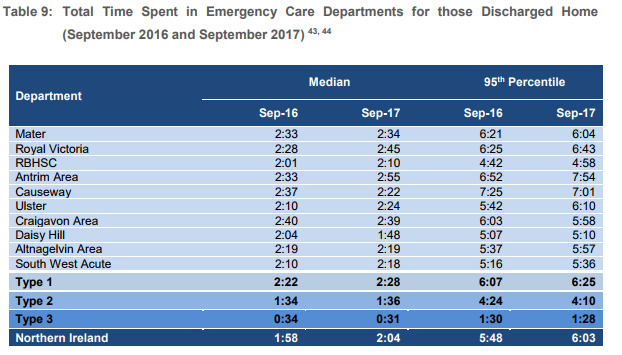
This would support the idea that people who do not need admitted are moving faster through the system than those who need admitted and the main issue in A&E is acutely ill patients needing a hospital bed
We are seeing increase activity in our main emergency departments for 2 reasons: 1) we have centralised serves to the main sites and shut down bed or alternative capacity, 2) the increase in population will see an increase in service users.
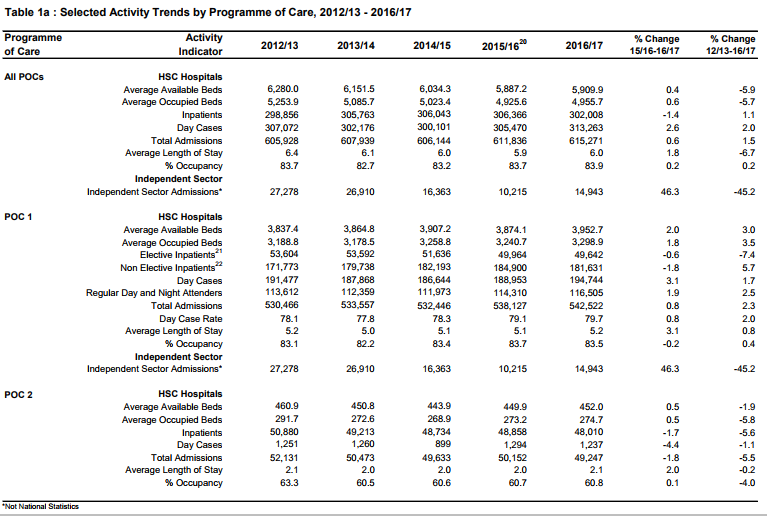
Below we see a table for the past 5 years for admission, across all our sites this is broadly in line with population rises and longer life expectancy.
Below we see a table for the past 5 years for admission, across all our sites this is broadly in line with population rises and longer life expectancy.
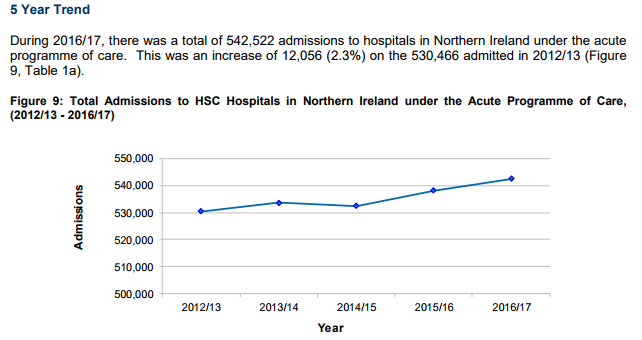
Now here comes the interesting part, while we see an increase in admission we also see a decrease in the length of stay, which in essence should create more bed space.
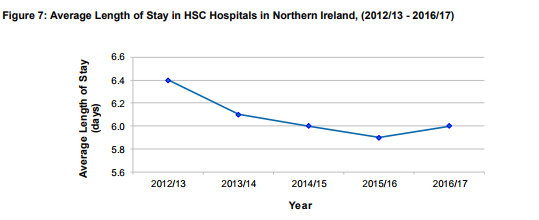
The crux though is that we have less beds in our system, the work done to create shorter stays in hospital and the increase in day cases meaning no overnight stays for small procedures is being undone cutting the amount of beds in our system.
Is Bengoa the answer, reform is needed no doubt of that but there have been several service changes ( https://www.health-ni.gov.uk/sites/default/files/publications/health/hs-niwts-ecwt-guidance.pdf page 12) in our emergency care since 2008, it seems to be forgotten that reform is happening all the time. Bengoa though like Transforming Your Care before it is a very subjective document that does not provide a plan, the framework is still being worked on and to all intensive purposes points towards more cuts and moving social care from the Trusts and moving to the English model of Local Authority based social care and be a step backwards for our health service in regards to this report https://ec.europa.eu/health/sites/health/files/state/docs/2017_companion_en.pdf .
An example of cuts to come using Bengoa and Michelle’s 10 year plan would be the removal of ambulatory care for children from Mid Ulster Hospital which will leave more sick children having to go to A&E in Antrim or Causeway and putting more pressure on the Emergency Care system http://www.northerntrust.hscni.net/pdf/Paediatric_Review_Consultation_Document.pdf
Be under no illusion while we have no Stormont Health Managers can let services fail or flourish, it seems to be that they let services fail to try and make a political statement, much like what they done during the summer when they announced massive cuts that were magically rescinded at the last minute.
From 2008 to 2013 we seen our health service fail amidst a series of reforms both contemporary and controversial, it’s not fair to say that there is no reform in our health service when there have been huge reforms:
Our performance now in 2017/18 is almost as bad as it was in 2012/13 when most of the above had taken place the moves we were told would make everything better. call me a traditionalist we need to look ahead at how we are going to deliver health services, sometimes though we have to look at what worked and we had a working system before the above changes were made, maybe our health planners need to step back and look at what worked and see how that can be brought into line with new forward thinking.
If we are serious about creating a template for health services it needs to be done on a white paper, the reason that past reviews failed and will also be the reason for Bengoa failing is that we are trying to build a health system on broken foundations by patching up the cracks. For example, would our acute A&E’s be located where they currently are if we were starting off with a blank sheet of paper? In the Northern Trust you could argue that Ballymena and Cookstown would be best placed for the main acute sites with network satellite hospitals in Antirm and Coleraine.
The answer won’t be found in advising people to use other services as it is people who need the hospital setting that are being held up in the system, increased triage systems at the mouths of A&E’s will help but ultimately won’t cure waiting times. Public announcements on social media or other formats have proven not to make a difference and telling GP’s not to refer patients is an insult to their profession. Neither will the answer be found in rushing patients to discharge to meet length of stay targets only for them to return via the A&E or blindly using clinical assessment units in A&E departments to try and free up space.
We either need bigger hospitals, more hospitals or what could be done return acute status to hospitals that were closed, everyone knows this managers, nurses, doctors and politicians and this widely know fact has widely been ignored all through Transforming Your Care and Bengoa and why one failed while the other is about to.
What we are seeing now with no Stormont is most certainly interesting with the creators of the 10 plan saying that we do not need an Executive to fix the health service, with a service in such a crisis if we do not need an Executive for this the question is do we need an Executive at all?
An example of cuts to come using Bengoa and Michelle’s 10 year plan would be the removal of ambulatory care for children from Mid Ulster Hospital which will leave more sick children having to go to A&E in Antrim or Causeway and putting more pressure on the Emergency Care system http://www.northerntrust.hscni.net/pdf/Paediatric_Review_Consultation_Document.pdf
Be under no illusion while we have no Stormont Health Managers can let services fail or flourish, it seems to be that they let services fail to try and make a political statement, much like what they done during the summer when they announced massive cuts that were magically rescinded at the last minute.
From 2008 to 2013 we seen our health service fail amidst a series of reforms both contemporary and controversial, it’s not fair to say that there is no reform in our health service when there have been huge reforms:
- Removal of acute A&E’s from Omagh, Belfast City, Mid Ulster and Whiteabbey
- Removal of acute inpatient beds from Omagh, Mid Ulster, Whiteabbey
- Opening of the South West Acute Hospital
- Opening of the New A&E in Antrim, with a new 24 bedded ward
- New Downe hospital opening
- Closures of Minor Injury Units
Our performance now in 2017/18 is almost as bad as it was in 2012/13 when most of the above had taken place the moves we were told would make everything better. call me a traditionalist we need to look ahead at how we are going to deliver health services, sometimes though we have to look at what worked and we had a working system before the above changes were made, maybe our health planners need to step back and look at what worked and see how that can be brought into line with new forward thinking.
If we are serious about creating a template for health services it needs to be done on a white paper, the reason that past reviews failed and will also be the reason for Bengoa failing is that we are trying to build a health system on broken foundations by patching up the cracks. For example, would our acute A&E’s be located where they currently are if we were starting off with a blank sheet of paper? In the Northern Trust you could argue that Ballymena and Cookstown would be best placed for the main acute sites with network satellite hospitals in Antirm and Coleraine.
The answer won’t be found in advising people to use other services as it is people who need the hospital setting that are being held up in the system, increased triage systems at the mouths of A&E’s will help but ultimately won’t cure waiting times. Public announcements on social media or other formats have proven not to make a difference and telling GP’s not to refer patients is an insult to their profession. Neither will the answer be found in rushing patients to discharge to meet length of stay targets only for them to return via the A&E or blindly using clinical assessment units in A&E departments to try and free up space.
We either need bigger hospitals, more hospitals or what could be done return acute status to hospitals that were closed, everyone knows this managers, nurses, doctors and politicians and this widely know fact has widely been ignored all through Transforming Your Care and Bengoa and why one failed while the other is about to.
What we are seeing now with no Stormont is most certainly interesting with the creators of the 10 plan saying that we do not need an Executive to fix the health service, with a service in such a crisis if we do not need an Executive for this the question is do we need an Executive at all?
 RSS Feed
RSS Feed
